
MYOPIA CONTROL
MYOPIA CONTROL FAQ’s
What is Myopia?
Myopia is blurry long-distance vision, often called “short-sighted” or “near-sighted”. A person with myopia can see clearly up close such as looking at their phone or reading a book, however viewing distance objects such as driving, copying from the blackboard or watching television can be blurry.
Myopia occurs when the eyeball grows too quickly in childhood, or when the eye continues to grow when eye growth should normally cease.
Why should I be concerned about myopia?
Myopia is becoming more common in children around the world. A recent study estimates that on average, 33% of the world is currently myopic and by 2050, based on current trends, almost 50% will be myopic. That’s a staggering 5 billion people! (source: Brien Holden Vision Institute) Developing myopia at a young age between 5-9 years means faster eye growth and this increases the chance of your child becoming highly myopic.
Higher levels of myopia are associated with higher risks of eye diseases such as:
- Myopic macular degeneration: Where the central vision deteriorates, like having a blur in the middle of your vision.

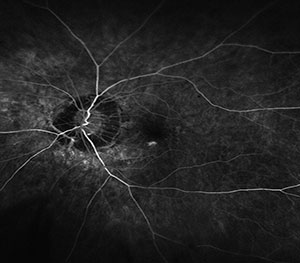
- Retinal detachment: Similar to a balloon getting thinner the more its being blown up, when the eyeball continues to grow the outer lining of the eyeball can get thinner and can result in a rip or tear. This can cause vision loss depending on its location

- Glaucoma: When the peripheral vision slowly deteriorates and in advanced cases can lead to tunnel vision and eventually complete blindness.

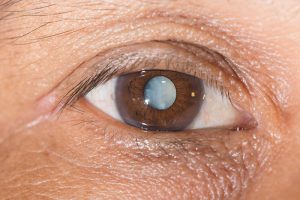
- Cataract: The lens inside the eye becomes cloudy, causing the vision to be blurry like looking through a dirty windscreen

What increases the risk of developing myopia?
- Age – Children from 5 to 9 years of age are more likely to develop myopia

-
- Ethnicity – Studies have shown that Asian ethnicity have a higher risk of developing myopia compared to European ethnicity.

- Genetics – Having one myopic parent increases the risk of your child becoming myopia by 3 times, and having two myopic parents increases the risk by 6 times.

- Time spent outdoors – Spending less than 1.5 hours a day outdoors with natural sunlight can increase the risks of developing myopia.

- Time spent indoors – Spending more than 2.5 hours a day on near tasks outside of school hours, such as reading, drawing, using smartphones and tablets can increase the risks of developing myopia.

How can I prevent myopia?
- Limit the time spent performing close up tasks (outside of school hours) such as reading, drawing, playing computer games, hand-held digital devices to less than 1.5 to 2 hours a day. The more time spent on near work, the higher the risks of developing myopia.

- Encourage more time spent outdoors with natural sunlight to 2.5 hours a day or more. Simple tasks such as walking the dog, sitting in the shade, playing in the park or backyard is sufficient as it is the brightness of natural sunlight that is beneficial. Sun protection precautions are recommended.

My child is already myopic, what can I do?
If your child is already myopic and there is a risk of further progression, it is recommended to implement Myopia Control to help slow down the rate of progression as much as possible.
The benefits of myopia control include:
- Improved long-term eye health by reducing risks of developing certain eye diseases
- Reduce risk of vision impairment
- Improved quality of life as supposed to wear thick and heavy spectacles as they reach high levels of myopia
- The different myopia control methods have approximately 40 – 60 % success rate, this means that there could still be some slight progression in some patients. However slowing down a child’s myopia by 50% is still a successful outcome as the risks of eye diseases in myopia of a child being -5.00D vs -6.00D increases exponentially.
- Research has shown that specialty contact lenses designs, orthokeratology and atropine eye drops have had the highest effect on slowing of myopic progression.
MYOPIA CONTROL OPTIONS
Orthokeratology
What is orthokeratology?
Orthokeratology (ortho-k) is a myopic control method that involves wearing a hard contact lens while sleeping in order to shape the front layer of the eyes.
Is orthokeratology safe for my child?
- Ortho-k is safe when the lenses are fitted correctly for your child’s eyes. Compliance with the aftercare schedules also ensure the lenses are working well and for any concerns to be addressed.
- Compliance with safety handling and maintenance of the lens will also minimise the risk of infections.
- Ortho-K is temporary and is not permanent, this means once your child ceases to wear ortho-k lens, the eye will slowly bounce back to its normal shape. Hence myopia control is more effective when the lenses are worn every night.
What are the benefits of orthokeratology?
- A benefit of ortho-k is in most cases the child does not require glasses or contact lenses during the day for vision correction. This means they are able to be spectacle-free which can be attractive for children who are very active in sports or are concerned cosmetically.
- Ortho-k lenses have a relatively long life. The lenses are recommended to be replaced every one to two years depending on their condition.
What are the concerns of orthokeratology?
- With all contact lens wear there is a small risk of eye infection. The likelihood of this could increase if safety hygiene and handling instructions are not followed.
- The fitting process for ortho-k is initially time consuming and requires commitment from both the child and the parents. There will be regular office visits for follow up care. After-care appointments will be scheduled in the morning for the first three months, and as a result the child may be required to be absent from school during this time. A medical certificate will be given to all students returning to school that day
Dual focus contact lenses
What is Misight / Multifocal soft contact lenses?
- These are specialty designed soft contact lenses that are worn full time to help slow down the progression of myopia.
- Misight lenses are daily disposable lenses that have been developed specifically for myopia control in children.
- Multifocal soft contact lenses have a similar design however they are replaced monthly.
What are the benefits of these lenses?
- Contact lens allow the child to be spectacle free which can be attractive if your child is active in sports or is concerned about the cosmesis of wearing spectacles.
- The MiSight lenses are daily disposables so they do not need to be cleaned after each use.
What are the concerns of these lenses?
- These lenses require an adaptation period of a few weeks depending on the child. Hence some children may experience slight visual blurring in the initial stages.
- With contact lens wear there is a small risk of eye infection. The risk of infections can be minimised if the patient is compliant with scheduled aftercares and instructions regarding hygiene and lens handling.
Compounded Atropine Eye Drops
What are atropine eye drops?
- Atropine eye drops are prescribed compounded eye medications instilled before bedtime every night for myopia control.
What are the benefits of atropine eye drops?
- Atropine treatment is easier to initiate and does not require many follow up appointments. The patient is seen one month after starting atropine and then at 3 months and then every 6 months thereafter.
What are the concerns of atropine eye drops?
- There could be some side effects in some patients such as eye allergies, mild blurring of near vision, stinging or itching.
- The patient will still require to wear spectacles or contact lenses in order to see.
Bifocals / Multifocals Spectacles
What are Bifocal or multifocal spectacles?
- These glasses have a distance zone and a near zone which is required to be worn full time in order to provide myopia control.
- They have a lower efficacy in myopia control compared to contact lens and atropine option.
What are the benefits of these spectacles?
They are less invasive than contact lenses or atropine.
What are the concerns of these spectacles?
- Bifocal spectacles have a horizontal line separating the distance and near zone. Some patients may be concerned of the cosmesis of bifocal spectacles.
- They may not be as effective at myopia control as contact lenses or atropine, however can still be considered in addition to atropine treatment.
Other FAQs about myopia control in children
Can my child get laser eye surgery to control myopia?
Laser eye surgery corrects myopia and eliminates the need to wear spectacles or contact lenses. Laser eye surgery is usually performed when the prescription is stable, which usually occurs when the child becomes an adult. Laser eye surgery does not slow the rate of myopic progression therefore it is still important to implement myopia control if the patient is still progressing.
Which myopia control method is best for my child?
Orthokeratology, dual focus soft contact lenses and atropine have higher efficacy in myopia control, followed by specially designed spectacles. After a comprehensive eye examination the optometrist will develop a tailored treatment plan for your child depending on your child’s needs. The best myopia control option is different for every child and is dependent on the factors below:
- Age
- Your child’s current prescription
- The shape of the front of their eyes
- Child/parent motivation and determination
- Maturity level
- Availability for regular office visits
Can my child’s treatment plan change?
The research on myopia control is constantly evolving and improving. Therefore as new evidence and treatments emerges we can modify your child’s treatment plan accordingly. Every child responds differently to myopia control, therefore if one particular treatment is not showing the expected effect we may change to another treatment or utilise a combination of treatments.
What is the earliest age to implement myopia control?
There is no minimum age to initiate myopia control. If a young child has become myopic and has high risk factors for progression then it would be in the child’s best interest to implement myopia control. The earlier the onset of myopia, the greater the risk of fast progression into higher levels of myopia. Hence early intervention is important in preventing high levels of myopia.
Can myopia control improve / reduce my child’s prescription?
Myopia occurs when the length of the eyeball increases or elongates. This process is irreversible and permanent. Myopia control will not reduce the length of the eye, it aims to reduce further elongation of the eye. This prevents further myopic progression and reduces the risks of certain eye diseases.
What is the length of treatment?
Myopia control should be continued throughout your child’s life where there is still risk of myopic progression without treatment. Typically myopia control is continued until early adult years or university years. Orthokeratology and soft contact lenses are safe for long term wear provided your child is compliant with their aftercares every 6 months. Atropine eye drops have a recommended treatment duration of 2 years, however there are studies conducted with atropine use for a 5 year period with minimal adverse effects.
Does wearing weaker glasses help with myopia progression?
There is a common misconception that wearing weaker glasses (undercorrection) will prevent myopic progression. Research shows that this is not the case and wearing weaker glasses does not inhibit progression but can actually increase progression especially if it is underprescribed.